Educational content on VJHemOnc is intended for healthcare professionals only. By visiting this website and accessing this information you confirm that you are a healthcare professional.
 A session with experts Marion Subklewe, Naval Daver, David Sallman, and Amer Zeidan, who discuss the latest immuno-therapeutic strategies in the treatment of acute myeloid leukemia (AML).
A session with experts Marion Subklewe, Naval Daver, David Sallman, and Amer Zeidan, who discuss the latest immuno-therapeutic strategies in the treatment of acute myeloid leukemia (AML).
![]()
Welcome to The AML Sessions brought to you by the Video Journal of Hematological Oncology (VJHemOnc). This exclusive discussion features leading experts Marion Subklewe, Naval Daver, David Sallman, and Amer Zeidan, who debate key updates in immuno-therapeutic approaches to AML.
The topics of discussion include checkpoint inhibitors in combination with hypomethylating agents in clinical trials, anti-CD47 therapy, bispecific antibodies (BiTEs) and CAR-T cell therapy.
Checkpoint inhibitors in combination with hypomethylating agents in clinical trials
“We can really see that there are some AML patients, where you do have good T-cell infiltration and good activation. And those were the ones who responded to treatments such as HMA PD-1, or PD-1-based treatment”
– Naval Daver
“I do think that we will see eventually some way for immune checkpoint inhibition in some capacity. Whether it’s in the post-transplant setting, whether it’s at the MRD level, but it sounds to me like we definitely need to do more work.”
– Amer Zeidan
Anti-CD47 therapy
“The excellent results or the promising at least very early data, if you think that CD47 is ubiquitously expressed. And, there’s a little bit higher expression maybe on AML, but it’s not a very specific target.”
– Marion Subklewe
Bispecific antibodies (BiTEs)
“We are actually working on a bispecific… Or bifunctional, antibody construct where we combine 47, for example, CD33 and CD123 in one construct.”
– Marion Subklewe
CAR-T cell therapy
“So I think there’s a lot of potential in immunotherapy. We just have to figure out which platform for which kind of patient, in which clinical situation and how to smartly combine. And I guess it’s still a lot of work ahead of us.”
– Marion Subklewe
Marion Subklewe:
So, hello. I’d like to welcome you to one of our AML sessions. So today we’re going to discuss AML in the context of immunotherapy. My name is Marion Subklewe. I’m a consultant in hematology at the LMU in Munich. And I’m very happy that I’m joined by three colleagues, so it’s Naval Daver from MD Anderson, it’s David Sallman from Moffitt, Florida, and I’m also joined by Amer Zeidan from Yale. So I’m very glad that you all joined. So also on this side of post-SOHO meeting, I think we like to discuss a few very interesting novel results of clinical trials that are currently running in the field of immunotherapy in AML. And I’d like to sort of structure our discussion on the different immunotherapy platforms. So we have the checkpoint inhibitors that on the one hand target several different checkpoint molecules and at the same time unleash endogenous immune responses.
Marion Subklewe:
We have the bi-specifics, where we have further advances in several clinical trials, and clearly there are also the CAR T-cells, very challenging in the AML fields. So I’d like to start with talking about the checkpoint molecules, and I’d like to ask my colleagues what they think, what’s currently the status, and where we are going. Maybe start with the checkpoint molecules that we already know from other entities before we then enter novel checkpoint molecules, where we have heard very interesting data at ASCO and also at the SOHO meeting. So maybe Naval, do you want to maybe start?
Naval Daver:
Sure. Thanks, Marion. So, pleasure to be here, and I think at the offset, there’s a lot happening in immunotherapy in AML compared to five, six years ago. So I think it’s an exciting area in general, in development with a number of different modalities. We’ve done a lot of work with the traditional immune checkpoints, the PD-1, PD-L1, CTLA-4-based therapies in numerous combinations, with hypometholating agents, with induction chemotherapy in maintenance. And I think that we are seeing some improvement in certain subsets, however, clearly not a blockbuster activity and not what we have seen in many of the solid tumors where we see very prolonged responses for years in some subset of patients.
Naval Daver:
So a lot of our biomarker work does seem to suggest that similar to the molecular heterogeneity in acute myeloid leukemia, there is also immune heterogeneity. And whether you look at it as degree of T-cell infiltration by numerically, or a percentage of bone marrow, or functionally. Which is even better, using single-cell cytokine analysis or other such modalities, we can really see that there are some AML patients, where you do have good T-cell infiltration and good activation. And those were the ones who responded to treatments such as HMA PD-1, or PD-1-based treatment. So I think if this is developed further, it has to be probably biomarker-driven, just like we do for FLT3, IDH, TP53, but I don’t think it’s a general scheme. Now, there may be one group of patients, such as post-transplant patients where there is very encouraging data with CTLA-4 inhibition showing some good responses, especially people with extramedullary disease. And at MD Anderson, we are kind of prioritizing extramedullary patients or those who are post-transplant for the CTLA-4 combination, CTLA-4 with HMA or CTLA-4 with PD-L1 with, or without HMA.
Naval Daver:
And we’re seeing some good responses in that population that we’ll hopefully update in the near future. But I think we need to find our own specific immune checkpoints. And I think there are some that are emerging that we’ll talk about more going forward, such as maybe TIM-3 on T-cells, maybe TIGIT and then a lot of work that David and me and others are doing with CD47, which is not T-cell but macrophage. So I think these will probably the ones to go forward and we can discuss them more.
Marion Subklewe:
Right. So, if you look at the list of clinical trials that are recruiting and checkpoints in combinations, mainly with hypometholating agents, but also with chemotherapy. I think there’s still a lot of data that’s going to be evolved and answer the questions, clearly monotherapy hasn’t shown any benefit, if anything, the combination. And I just wonder if you can comment on the trial, that was a negative on combining durvalumab in conjunction was hypomethylating agent and how you see this data compared to the data you generated in the MD Anderson.
Amer Zeidan:
Sure, and I think this is a great group. I think there was a wide representation of the several of the modalities that are being tested. I’d like to add a couple of things to what I think Naval mentioned, a one step back is that I think that the number of studies that have been done have first shown that these combinations are tolerable, are durable. In my experience, there has been a lot of hesitancy on myeloid investigators to use these type of drugs because of a couple of reasons. One of them is that the management of immune-mediated toxic reactions can be challenging, because you have often to do biopsies when you are dealing with pneumonitis. Its difficult to do a lung biopsy compared to a patient or solid tumor where we have good platelets, our patients are often low platelets. So doing biopsies to look for colitis for example, is challenging. And we often have fungal pneumonias and sometimes figuring out what you have is a pneumonitis versus a fungal infection, can be a challenge.
Amer Zeidan:
So there was a lot of hesitancy, I think originally, and my take on a lot of those first trials I would say is that the combinations are doable. There has been only one or two trials that show, I think a toxic signal, but for the most part, I think most of the other trials have shown that these drugs can be administered. As long as you monitor the patient carefully, intervene early with steroids and looking for adverse events. I do agree with Naval that I think overall, especially with monotherapy, the signal has been lacking. I think the combination trials have generally been somewhat mixed in their results. But one of the problems in general and the field has been, a lot of the trials that we’re enrolling, in my view, like single arm trials, enrolling frontline and relapse and a monotherapy and combination small numbers, those are rare cancers.
Amer Zeidan:
So it’s not like solid tumors where you have much bigger numbers. So I think sometimes it’s kind of tough when you add the degree of the immune landscape heterogeneity, between these patients to pick up exactly where you have to go. And I think this a randomized trial that you alluded to, the first randomized trial among both AML and MDS, but I think mostly for AML, all the unfit patients with AML in which patients received azacitidine or azacitidine with durvalumab, was negative in terms of both the primary endpoint, which was the response rate, but also in terms of the progression-free survival and overall survival. I think in this trial, the survival was in the range of 13 months for both arms, including the azacitidine monotherapy arm, which again in my mind, shows you the importance of doing these type of randomized trials. Because 13 months with monotherapy in older patients, if you look at historical control seven to eight months, if you did only the combination arm, you might think that there’s a signal, but when you look at the monotherapy I think it was realized that the signal is not necessarily there.
Amer Zeidan:
So I do think looking at biomarker driven approaches to try to select patients. Looking at rational designs of trials, rather than just combining whatever immune checkpoint inhibitor with whatever standard treatment we all use. And looking at novel checkpoints, like the CD47, that both David and Naval have done a lot of work with, as well as TIM-3 and LAG-3, and some of the other novel endpoints. I do think that we will see eventually some way for immune checkpoint inhibition in some capacity. Whether it’s in the post-transplant setting, whether it’s at the MRD level, but it sounds to me like we definitely need to do more work. And in collaboration between us as investigators, and industry to design the trials, and I think in the most informative way.
Marion Subklewe:
Yeah, absolutely. And I’d also just like to add that the mechanism of action of the checkpoint inhibitors might be also quite different, and we still don’t know exactly what the mode of action is. And if it’s maybe even depleting macrophages in the environment, or if it’s actually blocking interactions of T-cells, and so on. So also the mechanism of action might be quite different also depending on the type of AML or the different disease settings. So, I guess biomarkers are the way to go and understand mechanism of action, but, so many times now already CD47 has popped up. So I’m happy to give the word to David, and tell us a little bit about CD47 as the emerging star. Although, we’ve already seen very interesting data also in the lymphoma setting, so it’s been around for quite some time already.
David Sallman:
Yeah, sure. So I think as Naval alluded to earlier as well, I think now instead of talking about adaptive immunity, we’re talking about potentially unleashing innate. Although, there is clear correlations between innate and adaptive immunity then with 47 targeting. And I think pre-clinically several groups, although I think there’s a lot to grow from the translational perspective, so up regulation of 47. Both at higher risk MDS and acute myeloid leukemia, and at least in pre-clinical models, azacitidine can be synergistic with magrolimab by upregulating the pro “eat me” signals such as calreticulin. But I do think there’s probably a lot of data that’s going to emerge, I think retrospectively now based on the clinical responses that we’ve seen to date. I think now, through multiple presentations, again, most recently at EHA and ASCO, clearly, the combination has been, at least in high-risk MDS, quite transformative from at least the complete remission rate.
David Sallman:
And I think not just responses, I think we always have to look carefully at what the quality of the responses are. So there are very few marrow CR’s alone, almost all responses are either CR or some sort of marrow response in the setting of transfusion independence, or objective hematologic improvement. And clearly verses azacitidine therapy alone has been quite exciting, and that’s really leading up to the Phase III ENHANCE trial, which is launching, which is a double-blind placebo-controlled study of combination therapy versus azacitidine alone. Although, I think the significant interest similar to the venetoclax approval strategy in AML, are the response rates, can they support earlier approval, as the study continues to follow-up, I think importantly, and I think this is going to be shown with ongoing follow-up, but we’ve had median and follow-ups between six and ten months, depending on what subgroup you divide.
David Sallman:
And we’ve not had any median duration of response for overall survival, although clearly longer follow-up is quite critical. And then from translational and biomarker perspectives, we’ve not really had a group that’s predicted for poor responses really, across molecular subsets. But I think what we’ve been intrigued by is particularly p53 in AML, and we have amended the AML arm to basically preferentially enroll those patients. But across your 16 MDS and AML patients, we have about a 75% CR rate, most of those are AML patients. And again, more follow-up is needed, but the responses have been durable, and I would say exciting in that area to date
Marion Subklewe:
Right. Naval, do you want to comment from your experience?
Naval Daver:
Yeah, obviously very exciting. But the data is early, the numbers we have shown so far, but those are the numbers shown in the studies ongoing. So hopefully by ASH, there will be more updated data. To me, the most interesting is the activity in the TP53 AML, as David mentioned, that’s something that I don’t necessarily think we knew, a priori or mechanistically was something that we had. We would love to say we did, but it kind of just happened, we saw it, and the question still remains is, is the response really enriched in those patients? Or are we actually just seeing TP53 agnostic? Because, even a non-TP53, actually are doing well and the ASH abstracts will be out soon, and you’ll see the data, they actually do really well, survival wise.
Naval Daver:
So I actually think what’s happening is, you’re just not seeing as big an attrition in response, in survival with TP53. Maybe because the macrophages are not as impacted by the mutation as the molecular machinery, or even the T-cell machinery. For example, we looked at T-cells in TP53 mutated, and those had very poor function, cytokine production. So I think that’s very, very interesting, and of course then leads to the concept of, could you combine something like HMA-ven which has some activity does give you better response rates, 55, 60% compared to aza, with something like magrolimab. And then of course there’s also drugs like APR that are emerging for TP53. So I think the next year or two are going to be very interesting, to see how we can really improve the TP53 AML.
Naval Daver:
The other thing that I think is very interesting with this drug, especially given that we’re calling it an immune agent, is that we see almost no immunitis, and to me that is very, very intriguing. We’ve treated lots of BiTEs, you have them, we have them, we’ve used a lot of different PD-1, PD-L1, CTLA… You name it, they all have some degree of immune toxicity more or less. And with this agent, so far we’ve seen almost close to zero organ, IRIS or CRS. So to me, I think there’s some off target direct activity, that hopefully with a lot of correlative analysis, that’s ongoing will emerge. But that’s where we’re at right now.
Marion Subklewe:
The excellent results or the promising at least very early data, if you think that CD47 is ubiquitously expressed. And, there’s a little bit higher expression maybe on AML, but it’s not a very specific target. And I would have assumed from also pre-clinical and the lymphoma data that if anything, you need to combine with the targeting antibody construct. So I was actually very surprised, so we are actually working on a bi-specific… Or bifunctional, antibody construct where we combine 47, for example, CD33 and CD123 in one construct. As we were always assuming that monotherapy is, there’s going to be antigen sink and unspecific. So I’m also very amazed at this side effects, also hemolysis is something so far, better we haven’t treated any patients yet, but very manageable, right? So I was actually very surprised to see that.
David Sallman:
Yeah. I think it’s probably important to come at me. We do see this first cycle anemia, so we transfuse patients at higher thresholds, and there’s an average drop of a half a gram per deciliter. Although, there’s a range, and patients can have bigger drop, but what’s nice is typically by the end of cycle one, they’re close back to baseline and then really improve over time. And we’ve not had transfusion issues on patients, long-term on therapy, including patients out over a year in treatment. I do think again, how much is purely macrophage-mediated phagocytosis, and how much maybe LSC targeting. I think that’s a really key question I think in all of this. And I think that goes along with TIM-3 and some of the other markers too, how much has potentially LSC eradication. And I think really critical serial and single-cell studies need to be looked at from that question. But I do think there is a significant probably proportion that, that may be some of the importance.
Marion Subklewe:
Yes. Amer do you have any further comments or you want to use it in combination with PD-1, PD-L1 blockade?
Amer Zeidan:
No, I think I echo some of your comments. I actually worked with an anti-CD47, that was even before Magrolimab, so in some ways when the initial data was coming, I was along the lines of what you were saying. I was a little bit skeptical because the trial, it’s an agent called CC9-002 from Celgene, basically the trial enrolled 27, 28 patients. I treated 16 of them, so I’ve given a lot of this druf, we did not see any responses. I think later of course as we’ve done the translational data and negative studies, this is an abstract sitting in ASH 2019 library somewhere. Hopefully we can get the paper out at one point, but basically the translational data showed that there is, I think, which explains the lack of activities.
Amer Zeidan:
There was a lot of immunogenicity, so there was a lot of antibodies generated against the antibody itself. So I guess that also tells you that even… We tend to think of, for example, pembro and nivo, and all of these drugs as one in the same class. I think these are examples that it’s not only all anti-CD47’s are similar, there’s a number of other agents that are out there as well, basically at the ALX, I think, and Telerium. And I think it’s important that those should not be just treated equally, there could be differences in terms of how they induce responses. But also in terms of the other side of the CD47, which is the SIRP-alpha targeting, there are agents that are going after that as well. So I’m intrigued biologically as well, as you said, I don’t fully understand specifically, why is it so specific for myeloid malignancies, given that this is a uniformal, uniform mechanism across all cancers in terms of the CD40 expression and the TP53.
Amer Zeidan:
So it’s an interesting story, but in all honesty in AML and MDS, it’s not uncommon, we’ve been using lenalidomide forever without really understanding. And each two or three years, we get the new mechanism of action. So as long as the drug works, ultimately I think we would figure out how does it work, but I think sooner or later, with enough follow-up, I think we’ll have a very good sense of… I think with TP53, generally, I’m not as excited about responses. Because I do think we see responses, the problem is that patients often relapse and die. So I think if you have a solid survival signal, I think this drug would be a winner, so I just look for hopefully longer data. And as was mentioned, the randomized trials are already starting both in MDS and AML, so I think we are looking at a very robust program. So I’m pretty sure we’ll know for sure soon.
Marion Subklewe:
Yes, absolutely, I agree. I think the p53 is interesting because we know even after allo they have a detrimental outcome, and probably the bi-specifics and maybe even the CAR T-cells, there’s the topic of p53 and T-cell functions. So it might be, with a different mode of action, this might be less relevant. But we’ll see. So we’ll switch now to the bi-specifics, and I give myself two minutes for talking now, so I think the bi-specifics in AML have gone a more rocky road than we expected. So the translation from ALL to AML was more difficult maybe than expected, and most of the trials are still running and recruiting patients. And a lot of trials haven’t even achieved that the final and dose. So I think one of the issues in AML and the bi-specifics is finding a relevant serum concentration.
Marion Subklewe:
So I think it was very much misjudged that probably we have some kind of antigen sink. So if you look at the AMG 330 and the half-life extended AMG 673 trials, which we are involved in, one can see that currently we are applying 960 micrograms and in the blin we are with 28 micrograms already. So we clearly had a challenge and time was spent in moving up the dose. And the other thing is, that was probably expected, is that we do see cytokine release syndrome as the most common and highly relevant side effects. And currently the strategy, although nobody knows if this is actually the perfect strategy, is the dose step. So in the AMG 330 trial, we have now three dose steps, and are still moving up. And I think so far one can conclude that with this safety it’s okay. And CRS clearly also learning from the CAR T-cells with additional tocilizumab is manageable, but we still are challenged by seeing efficacy.
Marion Subklewe:
And I think two things have to be considered, first of all, that we still haven’t reached our final dose. And the second aspect is, most of the patients that have been included in these trials have a very adverse risk profile from cytogenetics. Half of them had been allogeneic transplantation, six median prior treatment lines. So it’s a really difficult challenge, so I think the very interesting part is that we are now moving in the MRD settings. So we are opening the cohort in AMG 330 for treating MRD patients, and clearly that’s also, again, similar to the blin data it’s a more suitable patient population. And this also comes back to what Naval at the beginning says, we need the AML cytogenetics and characteristics, but also we need some kind of immuno-fitness.
Marion Subklewe:
And I think it’s just not going to work in patients that are really far advanced in treatment line. And I think in that sense also, the half-life extended molecules might be easier, because we build up faster relevant PKs in the patients. So it might be easier to come up to a relevant dose in this patient cohort. And then I also think we’ll have adaptive immune escape mechanisms, so this will also bring us back to the checkpoint molecules. Where I really think we not only need to move early in treatment lines, but we definitely need also to combine as this can easily be observed. Also, from the patients treated that we have for up-regulation of PD-L1 as one of the obvious immune escape mechanisms. So I think there are a lot of different molecules running, we have the challenge of the right target antigen, we have the CRS, we have to cope. We are currently not in the wrong clinical situation and we probably also need some combination, I think, to get efficacy. So, that is my take. I don’t know who wants to comment.
Naval Daver:
Yeah, I can comment. We have a lot of these BiTEs ongoing, right at MD Anderson, many with you as well, Marion collaboration. I think the biggest issue is we haven’t moved to the right patient population, I don’t know why, and I know all of us have been talking to the companies. But I think really to test this, we have to go where the blinatumomab or the CAR-T in ALL have shown best activity, earlier salvage, you have T-cell fitness, low disease burden, and then maybe it’ll work, maybe it won’t. I don’t know, maybe it will still not work, but that’s really where blina, there’s a lot of data showing the CD8 to Treg ratio. The low disease burden, or at least averages as the best population. The second is, we are starting the combo with the PD-1.
Naval Daver:
And I think this way will be either go big or go home. We might get just tremendous CRS and it’ll shut down in 10 patients, or we may get tremendous CRS and 80% response like the CAR-T. And that’s what I keep whenever I discuss with the BiTE companies, because they say the magic solution. So I think you have to have one, either you have a response rate of 80% like the CAR-T in ALL and then I will do everything. I will admit the patient 25 days, toci, whatever, or you have a response rate of 30% like an IDH inhibitor and no toxicity almost, you cannot have 30, 35% and treat it like a CAR. So I think that’s what we’ll find out, that either low disease burden or the combo, is there a future for them? And hopefully we’ll know in like a year or so.
Marion Subklewe:
We’ve also seen the CAT T-cells, you can give the checkpoint day minus one, right? We were in the original clinical trials, but we now also get safety signals if you get it early, to get the T-cells moving. Right, I completely agree.
David Sallman:
I do think, just a caveat, I think translationally again, I think, thinking that we’re going to treat a all encompassing relapse/refractory patient population and have a good readout with any of these, I think is less likely. And so I think really the biology and looking at the T-cell infiltration and the markers, even 33, 123, are they, are they not, they also have their own toxicity. We have all these CAR-T trials, both 33, 123 open. And again, hopefully we’ll have some data over this next year. I think really, are these antigens worth targeting based on single antigen targeting, or do we critically need multiple target? Is it antigen escape? Is it more of a T-cell? Obviously we have auto and allo products that may help address that.
David Sallman:
To me, I want to see the efficacy and particularly the durable efficacy. I’m okay with responses, I think a lot of them have been very weak in how they’re presented and often the durability is very short. If I had a 20% CR, but it lasted for a year then I would be extremely excited, particularly if we could identify those patients. But I think trying to see that with these therapies… And then of course you can move it in all, in all the right settings, MRD, et cetera. But it’s still a long way to go, but at least there’s some efficacy out there. Hopefully we can make it better in the next year or so.
Amer Zeidan:
Yeah. And I think I would echo the same sentiment, I think some cautious optimism. I think one of the challenges with these agents have been the logistics. That 28 day infusion, nobody wants to do… There has been a lot of attempts to try to do longer-acting formulations. But when you look from a biological point of view, even at the blinatumomab and inotuzumab, which again, I think were major breakthroughs. But you get deep responses, MRD negativity, but the median survival is six months basically, or less, most patients are dying very quickly. And I think the ALL space is somewhat different, we have not had the same… Kind of things have flipped in the last few years. Like where AML have lagged behind for a long time. And then suddenly in the last three, four years you have nine drugs basically approved within the AML space.
Amer Zeidan:
And I wonder somewhat where the BiTEs are going to find their footing. I do think with those monotherapy results it’s really difficult, I do think that focusing on the right niche along the lines of what Naval was saying, basically on the MRD positivity analysis, I think you can show that really reducing this before transplant, for example, is going to prolong survival. I’m still not quite sure. What does it mean? Because again, it’s approved for blinatumomab for MRD positive to MRD negative disease, but I’m still not quite sure biologically, what does that mean? I may be… Maybe someone can update me, but I don’t think there has been data that just on the long run after transplant with blinatumomab, if you convert from MRD positive to MRD negative, that translates into longer survival. Because, we are probably not using the right way of looking at MRD. The level of sensitivity is probably different. So I do think those agents will need to have better strategic planning on where they should be positioned, and probably not on monotherapy.
Marion Subklewe:
Yes. So I think we’ll make a last round, we already started to do this, and just give everybody a chance to give his opinion on the CAR T-cells in AML. I think it was already addressed in a lot of the topics have been a clear overlap to the BiTEs. The target antigen, also the clinical situation, and I think it might be even more challenging was CAR T-cells. They very interesting data coming with NK constructs. So maybe Naval, you want to comment first?
Naval Daver:
Yeah, sure. I think we’re way behind in CAR T-cells from lymphoma and ALL, and I think it’s the same issue that we’ve discussed. That identifying optimal antigens is still something we haven’t been able to do for AML. So, we have a number of the constructs ongoing, they’re all in very early, Phase I, five or ten patients and no clear signal. So I know they’re new efforts and off-the-shelf, and combinations coming in, we will see in the next couple of years.
Marion Subklewe:
Yes. David, do you want to… You already commented on it, right?
David Sallman:
Yeah. I think not only is there a single antigen activity, yes, no. And then I think potentially looking at whether or not an allo product that likely needs more intense lymphodepletion, if that can improve this or some of the other novel technologies. That may get around some of the T-cell dysfunction that these patients likely intrinsically have. So I think hopefully we’ll have our like, foundation set over this next work. I do think my hypothesis is that, multi antigen targeted CARs and we really have to go for efficacy and not safety at this point, from my perspective, is important, but we’ll see.
Marion Subklewe:
Yeah. And I just want to comment one thing, I think it’s also important that we always realize the target antigen might not be the same, depending on what construct you are using in which epitope, which affinity, membrane, distance and so on. So it’s also important that we don’t burn target a ntigens just because of toxicity. I mean, it has to be taken seriously, but might be still quite different depending which construct we are actually using. And which co-stim domain and et cetera. Yes, I completely agree. Amer, do you want… Anything to say?
Amer Zeidan:
I think in addition to what was being said, I think the main issues with these, I think remain the toxicity. How do you limit the lives of those T-cells? I think those suicide genes or RNA-based T-cells or other approaches, and are you using these as a bridge to transplant?
Amer Zeidan:
Or do you have that tail of some patients, that have prolonged blasting responses similar to what was seen with ALL and diffuse large B-cell lymphomas? I think all of these are going to be very important questions as the clinical trials get conducted in terms of how those get positioned. But ultimately I think because of the manufacturing issues, and because of the high toxicity that need very specialized care and ICU care, these types of patients that are going to be very limited compared to the other things we talked about, like the BiTEs or the immune checkpoint inhibitor, which still is some experience, but I think the cellular therapy is even, a completely new level. And ultimately if we get those allogeneic CAR T-cells, kind of working, I think that would be a really a major breakthrough in my mind. So I think a very exciting field, but probably the least evolved so far, at least clinically compared to the other agents.
Marion Subklewe:
Absolutely, I completely agree. And I think there’s still a lot of work in understanding and identifying biomarkers, identifying suitable patients. But it just, that’s the last word I’d like to remind that immunotherapy is the most successful anti-leukemic, treatment, as we’ve seen an allogenic stem cell transplantation. So I think there’s a lot of potential in immunotherapy. We just have to figure out which platform for which kind of patient, in which clinical situation and how to smartly combine. And I guess it’s still a lot of work ahead of us. So with this, I’d like to thank you for this really nice discussion, and thank the audience for listening and looking forward. Probably next update we’ll have after ASH and see you along.
Amer Zeidan:
Thank you.
David Sallman:
Thank you for the discussion.

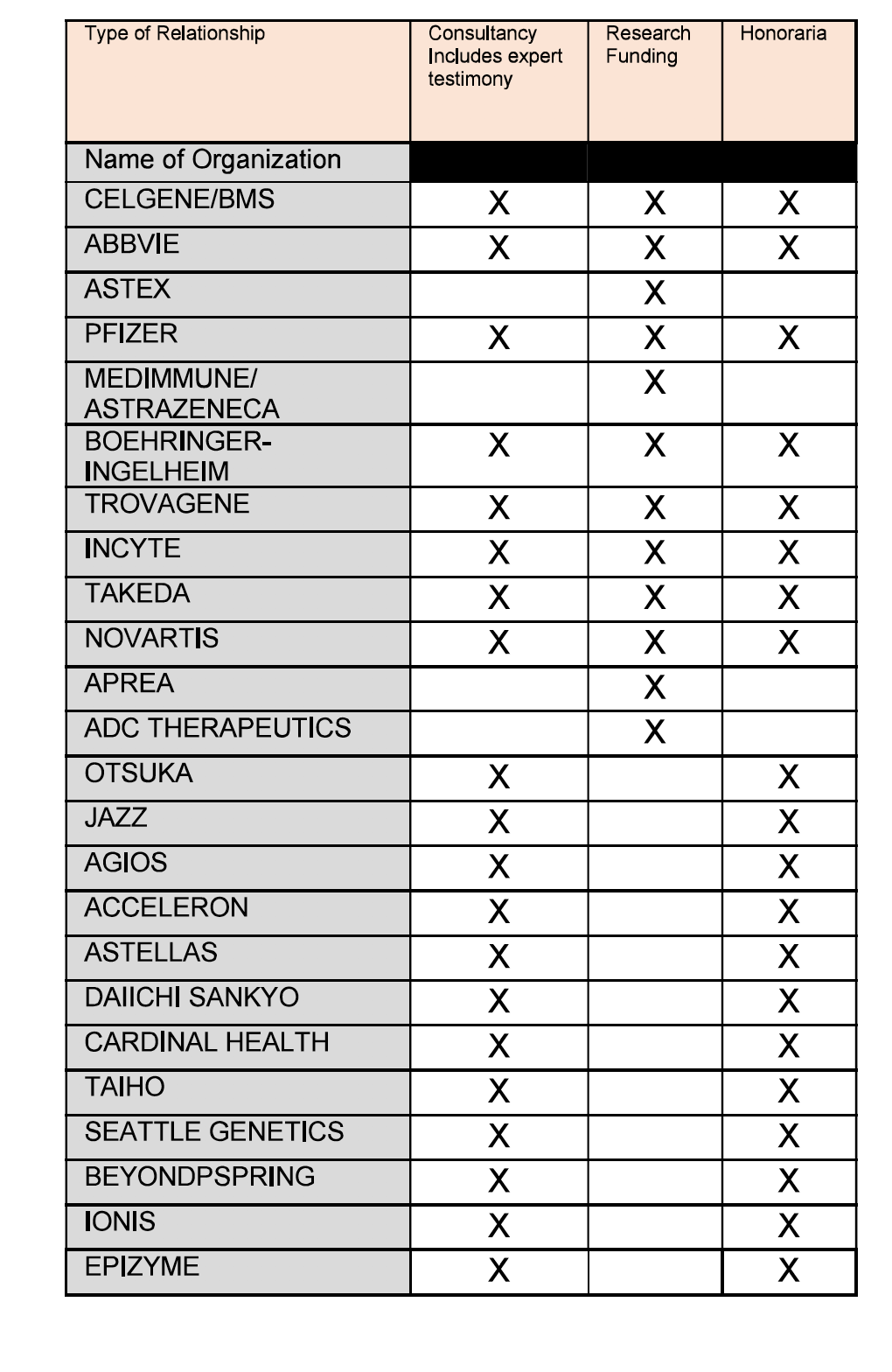
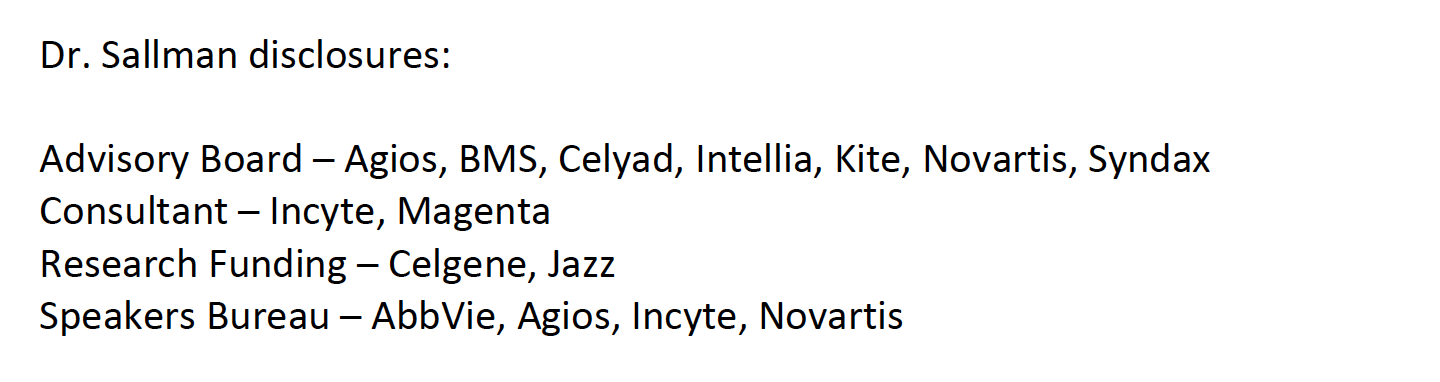
Disclosures
{kind=link}
{kind=link}
{kind=link}